
"Discount aldara uk, skin care reviews".
By: Z. Topork, M.B.A., M.B.B.S., M.H.S.
Program Director, Cooper Medical School of Rowan University
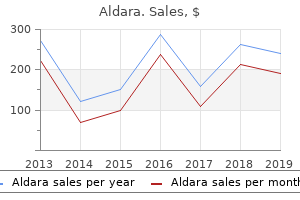
Deployment Validations Fifteen of the 19 cases had posttreatment image data that could be used for validation analysis acne prescription medication purchase aldara in india. Figure 2 shows 6 pairs of clinical and simulated deployments and presents them in ascending order according to their difference in device length acne hyperpigmentation order on line aldara. Most aneurysms were located on the internal carotid artery acne extractions order aldara with mastercard, and only 2 of the 19 aneurysms were fusiform acne under the skin buy aldara 5percent with mastercard, while the remaining were saccular. Physician Responses Table 2 presents the results of the surgical-planning questionnaire. Their comments on simulation utility in the questionnaire said that the simulations were specifically useful for the following: 1) rehearsing the deployment strategy and positioning of the device, 2) predicting how the device would behave around curved regions in the vessel, and 3) narrowing the list of device sizes being considered. Responses also indicated that the simulations increased perceived confidence in device selection in 94. Some physicians commented that they became more confident that the selected device size would span the desired proximal and distal landing points after viewing the simulation results. After viewing the simulation results, physicians selected a device size that was different from the originally planned device size in 63. In most of those cases (9/12), physicians selected a device diameter or length that was 1 size smaller or larger than the originally planned device size. Furthermore, a different device diameter was selected in half of the cases (6/12), while only a different device length was selected in the remaining half. Physicians perceived that the simulations reduced the number of devices used and operative time in 10. Seventeen of the 19 cases were treated with a single Pipeline device, while only 2 cases were treated with 2 Pipeline devices (ie, telescoping configuration). In 1 case, complete occlusion of the internal carotid artery with recanalization was observed, and in the second case, cerebral vasospasm was encountered. Regarding the procedural times of the 19 cases (quantified at the time from puncture until complete deployment), 6 cases were,30 minutes, 1762 Chong Oct 2019 The deployment pairs are sorted in ascending order according to the difference between actual and simulated device lengths, which ranged from 1. The plots show the means for the deployment pairs on the x-axis and the differences between pairs on the y-axis. After viewing simulation results, the participating physicians changed their device size selections in 63. This result highlights the impact of computational modeling on treatment planning. Physician responses indicated that the effects of computational modeling on the number of devices used and on procedural time were limited to a small percentage of cases. However, such effects may be difficult to observe on the basis of a questionnaire, given a small sample size. A planned future study will use a larger patient population and a control group to better elucidate the influence of computational modeling on the number of devices used and procedural time. To our knowledge, this is the first study that evaluates the utility of computational device modeling in a prospective case series. Many studies have been reported in the literature on the application of computational device modeling to treatment planning. Yet, evaluations under typical clinical workflows are essential for understanding the contribution of the technology to clinical practice and its potential for adoption. First, the study included a small sample of patient cases and a small number of physicians. We did not think that it was justified to repeat the imaging and thereby expose the patients to additional unnecessary radiation. Furthermore, the primary goal of the study was to gauge the impact of computational modeling on clinical workflows, and a sample size of 19 was deemed appropriate for this purpose. Future work will include evaluating the impact of computational modeling on a larger patient population with a control group. Second, the distribution of cases among physicians was skewed, and most cases (73.
A randomized trial of cryo stripping versus conventional stripping of the great saphenous vein skincarerx discount aldara generic. Duplication of the great saphenous vein: a definition problem and implications for therapy acne jensen boots sale order generic aldara online. Meta-analysis of transilluminated powered phlebectomy for superficial varicosities acne denim buy aldara once a day. Long-term outcomes of endovenous radiofrequency obliteration of saphenous reflux as a treatment for superficial venous insufficiency acne zits generic 5percent aldara overnight delivery. Endovenous ablation (radiofrequency and laser) and foam sclerotherapy versus open surgery for great saphenous vein varices. Randomized clinical trial comparing two methods for endovenous laser ablation of incompetent perforator veins in thigh and great saphenous vein without evidence of saphenofemoral reflux. Endovenous laser treatment of the lesser saphenous vein with a 940-nm diode laser: early results. Infrequent early recanalization of greater saphenous vein after endovenous laser treatment. Early results and feasibility of incompetent perforator vein ablation by endovenous laser treatment. Randomized clinical trial comparing endovenous laser ablation, radiofrequency ablation, foam sclerotherapy and surgical stripping for great saphenous varicose veins. Randomized trial comparing endovenous laser ablation of the great saphenous vein with high ligation and stripping in patients with varicose veins: short-term results. Endovenous thermal ablation of superficial venous insufficiency of the lower extremity: single-center experience with 3000 limbs treated in a 7-year period. Advances in laser surgery for leg veins: bimodal wavelength approach to lower extremity vessels, new cooling techniques and longer pulse durations. Systematic review of outcomes after surgical management of venous disease incorporating subfascial endoscopic perforator surgery. Neovascularisation and recurrence 2 years after varicose vein treatment for sapheno-femoral and great saphenous vein reflux: a comparison of surgery and endovenous laser ablation. Treatment of incompetent perforating veins using the radiofrequency ablation stylet: a pilot study. Conservative versus surgical treatment of venous leg ulcers: a prospective, randomized, multicenter trial. A prospective study of the fate of venous leg perforators after varicose vein surgery. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. Multi-society consensus quality improvement guidelines for the treatment of lower-extremity superficial venous insufficiency with endovenous thermal ablation from the Society of Interventional Radiology, Cardiovascular Interventional Radiological Society of Europe, American College of Phlebology and Canadian Interventional Radiology Association. Recommended reporting standards for endovenous ablation for the treatment of venous insufficiency: joint statement of the American Venous Forum and the Society of Interventional Radiology. Endovenous ablation (radiofrequency and laser) and foam sclerotherapy versus conventional surgery for great saphenous vein varices. Randomized clinical trial of endovenous laser ablation versus conventional surgery for small saphenous varicose veins. Revision of the venous clinical severity score: venous outcomes consensus statement: special communication of the American Venous Forum Ad Hoc Outcomes Working Group. It is not intended to be a recommendation of one product over another, and is not intended to represent a complete listing of all products available. Clarified medically necessary statement for junctional (saphenofemoral or saphenopopliteal as appropriate based on vein anatomy) incompetence. Mechanochemical ablation of any vein added as an investigational and not medically necessary statement. Medically necessary and investigational and not medically necessary criteria revised to address saphenofemoral and saphenopopliteal junction incompetence and endoluminal cyoablation.
These submicroscopic rearrangements may account for a sizable portion of the human genetic disease burden acne whiteheads buy aldara 5percent, with some estimates as high as 15% (10) skincare for 25 year old woman purchase aldara in india. The probability of finding significant copy number variants is highly correlated with the presence of structural fetal abnormalities skin care jogja buy aldara with visa, although significant copy number variants also can be identified in structurally normal fetuses skin care qualifications order 5percent aldara amex. This can occur between two different individuals or between paired chromosomes of the same individual and may or may not cause disease. Although both of these techniques detect copy number variants, they identify different types of genetic variation. Duplications or deletions are detected as regions with a higher or lower hybridization signal than the control sample. Arrays also can be "targeted" and focus on copy number variants of known pathogenicity instead of testing the entire genome. Targeted arrays are designed to primarily detect copy number variants known to cause clinical findings, while minimizing the detection of variants of uncertain clinical significance. In contrast, wholegenome arrays are designed to provide greater coverage across the genome and, tl1erefore, optimize detection, but may be more likely to identify differences that have uncertain clinical consequences. Because such a large number of potential findings are possible with any type of microarray technology, databases are used to determine if specific copy number variants have been previously reported and whether they are considered pathogenic, benign, or of unknown significance. Chromosomal Microarray Versus Karyotype the primary advantage of chromosomal microarray analysis over the conventional karyotype is the higher resolution, which yields more genetic information. Because chromosomal microarray analysis does not require dividing cells, it may be useful in the evaluation of fetal demise or stillbirth, in which the culturing of macerated tissue is frequently unsuccessful (11). In addition, chromosomal microarray analysis is a standardized procedure that involves the use of computerized analysis, whereas karyotyping involves microscopic examination of stained chromosomes and may be more subjective and prone to human error. Unlike conventional karyotyping, chromosomal microarray analysis cannot detect balanced inversions, balanced translocations, or all cases of tissue mosaicism. In addition, not all microarrays can detect triploidy, although most triploid fetuses can be identified by ultrasonography. In some cases, the significance was uncertain because the findings were rare or novel, whereas son1e results were known to have variable penetrance. That is, such results indicate a susceptibility to a particular outcome, such as autism, but not a certainty that this will occur. In some cases, evaluation of parental samples can help clarify whether or not this is an inherited finding or a new finding in the offspring; however, the clinical outcome may remain unclear. Of note, the interpretation of many such results changed over tl1e course of the study as additional information became available regarding the significance of some copy number variants. Thus, interpretation of results is expected to improve as knowledge of the human genome grows and the use of databases to link clinical findings with copy number variants becomes more robust. The test may identify consanguinity (a close blood relationship or incest) or nonpaternity. Samples from both parents may be required to help understand the significance of these results. Test results may identify adult-onset diseases that will not affect health during the newborn period or childhood but may have unknown severity later in life. Identification of such findings may also indicate that one of the parents has the same adult-onset disease but has not yet developed symptoms. The potential for detection of clinically uncertain and co1nplicated findings with prenatal chromosomal microarray analysis can result in substantial patient anxiety. This underscores the critical need for comprehensive patient pretest and posttest genetic counseling from qualified personnel such as a geneticist or genetic counselor about the benefits, limitations, and results of testing so that patients can make informed decisions. Information that should be shared with patients who are considering prenatal chromosomal microarray analysis is provided for use before referral for genetic counseling (see Box 1). In general, the women reported a need for extensive support and counseling regarding the analysis. In addition, some types of arrays can identify evidence of consanguinity and nonpaternity. The type and amount of information reported varies depending on the type of array used as well as the policy of the laboratory that performs the analysis (14). Therefore, genetic counseling and informed consent is essential before patients undergo testing -with this technology. Recommendations the College and the Society for Maternal-Fetal Medicine offer the following recommendations for the use of chromosomal microarray analysis in prenatal diagnosis: In patients with a fetus with one or more major structural abnormalities identified on ultrasonographic examination and who are undergoing invasive prenatal diagnosis, chromoson1al microarray analysis is recommended.
If iodine deficiency exists during this period and results in thyroid hormone deficiency skin care 30s order aldara without a prescription, the consequence is derangement in the development of brain and central nervous system acne 2 weeks pregnant purchase aldara us. These derangements are irreversible skin care equipment suppliers order aldara 5percent visa, the most serious form being that of cretinism acne 24 purchase aldara american express. The effect of iodine deficiency at different stages of life is given in Table 34 (2). The other physiologic role of thyroid hormone is to control several metabolic processes in the body. For example, thyroid hormone increases energy production, increases lipolysis, and regulates neoglucogenesis, and glycolysis. However, pregnant women, lactating women, women of reproductive age, and children younger than 3 years are considered to be at high risk (3). During foetal and neonatal growth and development, iodine deficiency leads to irreversible damage to the brain and central nervous system. Dietary sources the iodine content of food depends on the iodine content of the soil in which it is grown. The iodine present in the upper crust of earth is leached by glaciation and repeated flooding and is carried to the sea. The seaweed located near coral reefs has an inherent biologic capacity to concentrate iodine from the sea. Thus, a population consuming seaweed and reef fish has a high intake of iodine, as the case in Japan. The average iodine content of foods (fresh and dry basis) as reported by Koutras et al. Thus, the average iodine content of foods shown in Table 35 can not be used universally for estimating iodine intake. However, more recent data indicate that the iodine content of human milk varies markedly as a function of the iodine intake of the population. The iodine requirement of pre-term infants is twice that of term infants because of a 50 percent lower retention of iodine by pre-term infants. Such values have been observed in iodine-replete infants in Europe (11), Canada (12), and the United States (12). Table 36 Iodine content of the inorganic world Location Terrestrial air Marine air Terrestrial water Sea water Igneous rocks Soils from igneous rocks Sedimentary rocks Soils from sedimentary rocks Metamorphic rocks Soils from the metamorphic rocks Iodine content 1. These requirements are based on the body weight of Mexican children who participated in this study. The average body weight of a 10-year-old child, as per the Food and Agriculture Organization references, is 25 kg.
Aldara 5percent with mastercard. 😱10 Skincare Mistakes That Make Your Acne Worse & Sensitize Your Skin!.