
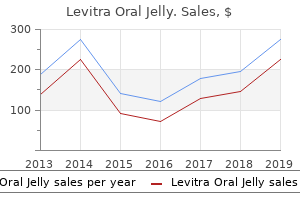
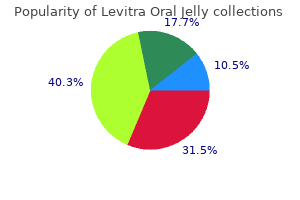
"Buy levitra oral jelly with american express, erectile dysfunction pills australia".
By: V. Daro, M.B. B.CH. B.A.O., Ph.D.
Deputy Director, Marian University College of Osteopathic Medicine
These methods can be equally used to noninvasively study brain structure and function in preclinical laboratory models erectile dysfunction symptoms treatment cheap levitra oral jelly 20mg overnight delivery, and the ability to derive identical metrics of brain structure and function from the bench to the bedside is a key benefit of neuroimaging methods for translational research erectile dysfunction after age 40 discount generic levitra oral jelly canada. Analogous neuroimaging methods are also increasingly being applied to ex vivo studies (of autopsied brain tissue) so that the three-dimensional structure of the brain can be assessed at microscopic resolution without the disruption and distortion caused by sectioning for staining and analysis by standard microscopy impotence problems purchase levitra oral jelly online from canada. Finally causes of erectile dysfunction in youth cheap levitra oral jelly online, over the past decade, there have been remarkable advances in optical microscopic methods that allow cellular structure and function to be visualized in vivo. Neuroimaging methods are enabling researchers to identify neural networks involved in cognitive processes, understand disease pathways, recognize and diagnose diseases early when they are most effectively treated, and determine how therapies work. As in other areas of biomedical research, these opportunities are closely intertwined. As an example, imaging can provide a better understanding about a disease process that leads to discovery of potential therapies that intervene in that process. Thereafter, imaging can help provide a better understanding about how that drug or therapy works at the physiological-molecular level, leading to a more precise understanding of the disease process and then to the development of a more highly specific drug to treat it. A range of imaging methods are used to reveal brain structure (anatomy), physiology (functions), and biochemical actions of individual cells or molecules. The three main categories, therefore, are often referred to as structural, functional, and molecular imaging. While most imaging techniques have applications throughout the body, the descriptions provided in this monograph focus on their use in the nervous system, primarily the brain. Alone and in combination, these imaging techniques are transforming our understanding of how the brain functions, how immune cells function, and how immune cells interact with the brain in health and disease. Links to more detailed descriptions of the work being conducted in these selected neuroimaging research projects are provided in the brief highlights of the research in this monograph. The photons were initially recorded onto a silver halide film as they passed out of the body. X-rays of the head provided limited information about the brain, however, since brain parenchyma (the functional tissue) is far less radiodense than the skull. Locations of calcified structures such as the choroid plexae and pineal gland, though, might be visible and seen to be displaced by a putative mass lesion. The pneumoencephalogram examined x-rays of the head after replacing the spinal fluid with air or another gas which allowed the ventricular outlines to be detected, again as a way of assessing for symmetry or its disruption. Angiography, a related early technique, uses radiodense dye injected through a catheter into a blood vessel to detect a blockage or narrowing of downstream vessels, or other vascular lesions such as aneurysms or arteriovenous malformations. Angiography is used to visualize arteries anywhere in the body, including the neck and brain. Although angiographic data are now digitized and analyzed using algorithms that subtract pre-contrast and post-contrast images (termed "digital subtraction angiography"), this method still provides the highest resolution images of vascular structures in the brain and remains in wide clinical use. Cormack and Sir Godfrey Newbold Hounsfield) received the Nobel Prize in Medicine or Physiology in 1979. This technology uses special x-ray equipment to obtain and reconstruct three-dimensional anatomical images of bone, soft tissues, and air in the entire body, including the head. Electronic sensors measure the amount of radiation that is absorbed by different tissues and a computer analyzes variations in x-ray absorption across angles to form cross-sectional images or "slices" of brain called "tomograms. Mass lesions are also visible either directly as a change in tissue density and/or indirectly through the compression of adjacent brain structures, as well as by their enhancement after contrast administration. These include subtle hypodensity, loss of normal differentiation between gray matter and white matter, and subtle mass effect. Tiny blood clots could also sometimes be detected at the location of major brain arteries. Ultrasound, another early technique developed in the 1930s-40s, was primarily used neurologically until the 1960s to try to identify brain tumors. Ultrasound uses sound waves to determine the locations of surfaces within tissues and differentiates surfaces from fluids. It does so by measuring the time that passes between the production of an ultrasonic pulse and the echo created when the surface reflects the pulse. Ultrasound remains a valuable brain imaging technique in neonates where signals can be reliably obtained through the fontanelle.
Besides impotence at 37 buy levitra oral jelly 20 mg low cost, it may have been caused by inferior imaging techniques and interpretations erectile dysfunction doctors in pa best purchase for levitra oral jelly. The initial symptom(s) at presentation could be retrieved in 58 patients; a majority of the patients (n=34 erectile dysfunction doctors in maine discount levitra oral jelly 20mg on line, 58%) presented with multiple symptoms erectile dysfunction vacuum therapy discount 20 mg levitra oral jelly fast delivery. Eight patients presented with other audiovestibular symptoms: vertigo, unsteadiness or tinnitus. Two patients are not shown, of which one had no complaints and was diagnosed through cascade screening and the other had bilateral vestibular schwannomas that were coincidentally identified on imaging. Kokkinou, Athens Medical School, Special Unit of Pediatric Neurology, First Department Of Pediatrics Background: Neurocutaneous syndromes are a group of congenital disorders that include abnormalities of neuroectodermal and, sometimes, mesodermal development. A multidisciplinary approach to care has been advocated in order to provide optimum care for these complex disorders. Methods: Patients were evaluated by a multidisciplinary team of specialists, including pediatric neurologist, dermatologist, oncologist, ophthalmologist, geneticist, orthopedist, neuroradiologist and psychologist. Establishment of a multidisciplinary center for neurocutaneous disorders can improve clinical care by providing multidimensional approach and contributing to early diagnosis and timely therapeutic intervention. This situation is the reason of emotional disturbances, and the need for psychological support. Emotional functioning was assessed based on interview with parents, psychological investigation and observation of the patients. Data of 50 pts were completed and analyzed using some subscales of Vineland Adaptive Behavior Scales second edition. We assessed social competence of patients, like: cooperativeness, interpersonal appropriates, recognizing social cues, following social rules. We assessed also maladaptive behavior in this population as a risk of social rejection, especially ability to controlling anger, tendency to impulsive behavior, temper tantrums, lack of considerations, strange habits or ways, bizarre speech etc. Results: In our group of patients we do not observe higher level of difficult behaviors (maladaptive behavior). Specific for these children are expressive emotionality and open communication of their needs. As additional factors we found physical appearance (cafй au lait spots, freckles, neurofibromas in visible parts of the body). Few studies have actually aimed to establish the role of medical imaging in the management and follow-up of these patients. Various clinical manifestations and complications, relevant personal characteristics, family history and results from genetic testing were also collected from their electronic records. Results: All 70 patients presented cutaneous neurofibromas and cafй au lait spots. Of them, 58% of mutations were substitutions; 32% deletions; 8% duplications; 2% insertions. Studies on larger cohorts will have to be done to lead to significant conclusions. Full List of Authors: Remy Lamontagne*1, 2, Rahma Derbel3, Vincent Roy1, 4, Hйlиne T. Although these tumors are uncommon in childhood and asymptomatic in most cases, careful observation is required for them. One patient had a severe plexiform neurofibroma affecting the whole body and underwent debulking surgery. Another patient had pilocytic astrocytoma and malignant peripheral nerve sheath tumor in the mediastinum at age of 9 years. One patient with an age of 32 years needed debulking surgery due to severe plexiform neurofibroma of the head and neck. Peripheral and plexiform neurofibroma were most commonly discovered in lower extremities and paravertebral spaces. The trend towards high numbers of patients having height < 5th percentile was similar when patients with history of optic pathway glioma were excluded. Detailed clinical and molecular (blood and melanocyte) testing information was available, reviewed and recorded in a dedicated database. Statistical analysis was performed for trait distribution differences among groups. In 1/5 the test was non-conclusive and biopsy sites on the anterior chest developed undesirable hypertrophic scars.
However erectile dysfunction pills that work generic levitra oral jelly 20mg, it may be seen in some waking patients with neurodegenerative disorders fast facts erectile dysfunction buy 20mg levitra oral jelly. Ventilatory patterns erectile dysfunction questions to ask discount generic levitra oral jelly canada, with the exception of psychogenic hyperventilation erectile dysfunction chicago best order for levitra oral jelly, are normal. In some patients with psychogenic coma, the eyes deviate toward the ground when the patient is placed on his or her side. Most patients with metabolic brain disease have diffusely abnormal motor signs including tremor, myoclonus, and, especially, bilateral asterixis. The patient with gross structural disease, on the other hand, generally has abnormal focal motor signs and if asterixis is present, it is unilateral. Finally, metabolic and structural brain diseases are distinguished from each other by a combination of signs and their evolution. Most conscious patients with metabolic brain disease are confused and many are disoriented, especially for time. Their abstract thinking is defective; they cannot concentrate well and cannot easily retain new information. Early during the illness, the outstretched dorsiflexed hands show irregular tremulousness and, frequently, asterixis. Posthyperventilation apnea may be elicited and there may be hypoventilation or hyperventilation, depending on the specific metabolic illness. By contrast, awake patients with psychogenic illness, if they will cooperate, are not disoriented and can retain new information. The orderly rostral-caudal deterioration that is characteristic of supratentorial mass lesions does not occur in metabolic brain disease, nor is the anatomic defect regionally restricted as it is with subtentorial damage. Neurons and glial cells undergo many chemical processes in fulfilling their specialized functions. The nerve cells must continuously maintain their membrane potentials, synthesize and store transmitters, manufacture axoplasm, and replace their always decaying structural components (Figure 52). In addition, they may aid neuronal function by supplying substrate (lactate)51 (although the degree, if any, to which neurons metabolize lactate in vivo is controversial53). Astrocytes also participate in controlling blood flow52 and in maintaining the blood-brain barrier. Awake or asleep, the brain metabolizes at one of the highest rates of any organ in the body. However, although the overall metabolism of the brain is relatively constant, different areas of the brain metabolize at different rates, depending on how active an area is. These considerations are central to an understanding of many of the metabolic encephalopathies, and the following paragraphs discuss them in some detail. Overall flow in gray matter, for example, is normally three to four times higher than in white matter. At glutamatergic synapses, presynaptically released glutamate depolarizes postsynaptic neurons by acting at specific receptor subtypes. The action of glutamate is terminated by an efficient glutamate uptake system located primarily in astrocytes. Lactate, once released by astrocytes, can be taken up by neurons and serves them as an adequate energy substrate. A functional magnetic resonance imaging scan of the normal individual flexing and extending his fingers. Blood flow increases to a greater degree than oxygen consumption in the motor areas, leading to an increase in oxyhemoglobin. The paramagnetic oxyhemoglobin causes an increased blood oxygen level-dependent signal in the motor cortex bilaterally. The increase in glucose metabolism over oxygen metabolism results in increased lactate production, possibly the substrate for the increased demand of neurons58 (Figure 54). Important among these are adenosine, nitric oxide, dopamine, acetylcholine, vasoactive intestinal polypeptide, and arachidonic acid metabolites. Examples of such reactive hyperemia or ``uncoupling' of flow and metabolism occur in areas of traumatic or postischemic tissue injury, as well as in regions of inflammation or in the regions surrounding certain brain tumors.
These spinal level motor patterns may occur in patients with severe brain injuries or even brain death impotence surgery buy levitra oral jelly 20mg on line. Failure to withdraw on one side may indicate either a sensory or a motor impairment what age does erectile dysfunction happen levitra oral jelly 20 mg, but if there is evidence of facial grimacing erectile dysfunction at age 28 purchase discount levitra oral jelly, an increase in blood pressure or pupillary dilation impotence hernia order levitra oral jelly with american express, or movement of the contralateral side, the defect is motor. Failure to withdraw on both sides, accompanied by facial grimacing, may indicate bilateral motor impairment below the level of the pons. Posturing responses include several stereotyped postures of the trunk and extremities. Most appear only in response to noxious stimuli or are greatly exaggerated by such stimuli. Seemingly spontaneous posturing most often represents the response to endogenous stimuli, ranging from meningeal irritation to an occult bodily injury to an overdistended bladder. The nature of the posturing ranges from flexor spasms to extensor spasms to rigidity, and may vary according to the site and severity of the brain injury and the site at which the noxious stimulation is applied. In addition, the two sides of the body may show different patterns of response, reflecting the distribution of injury to the brain. Clinical tradition has transferred the terms decorticate rigidity and decerebrate rigidity from experimental physiology to certain patterns of motor abnormality seen in humans. First, these terms imply more than we really know about the site of the underlying neuro- logic impairment. Even in experimental animals, these patterns of motor response may be produced by brain lesions of several different kinds and locations and the patterns of motor response in an individual to any one of these lesions may vary across time. In humans, both types of responses can be produced by supratentorial lesions, although they imply at least incipient brainstem injury. There is a tendency for lesions that cause decorticate rigidity to be more rostral and less severe than those causing decerebrate rigidity. In general, there is much greater agreement among observers if they simply describe the movements that are seen rather than attempt to fit them to complex patterns. Flexor posturing of the upper extremities and extension of the lower extremities corresponds to the pattern of movement also called decorticate posturing. The fully developed response consists of a relatively slow (as opposed to quick withdrawal) flexion of the arm, wrist, and fingers with adduction in the upper extremity and extension, internal rotation, and vigorous plantar flexion of the lower extremity. However, decorticate posturing is often fragmentary or asymmetric, and it may consist of as little as flexion posturing of one arm. Such fragmentary patterns have the same localizing significance as the fully developed postural change, but often reflect either a less irritating or smaller central lesion. The decorticate pattern is generally produced by extensive lesions involving dysfunction of the forebrain down to the level of the rostral midbrain. A similar pattern of motor response may be seen in patients with a variety of metabolic disorders or intoxications. For example, in the series of Jennett and Teasdale, after head trauma only 37% of comatose patients with decorticate posturing recovered. Some patients assume an opisthotonic posture, with teeth clenched and arching of the spine. Tonic neck reflexes (rotation of the head causes hyperextension of the arm on the side toward Examination of the Comatose Patient 75 which the nose is turned and flexion of the other arm; extension of the head may cause extension of the arms and relaxation of the legs, while flexion of the head leads to the opposite response) can usually be elicited. As with decorticate posturing, fragments of decerebrate posturing are sometimes seen. These tend to indicate a lesser degree of injury, but in the same anatomic distribution as the full pattern. It may also be asymmetric, indicating the asymmetry of dysfunction of the brainstem. Although decerebrate posturing usually is seen with noxious stimulation, in some patients it may occur spontaneously, often associated with waves of shivering and hyperpnea. Decerebrate posturing in experimental animals usually results from a transecting lesion at the level between the superior and inferior colliculi. The level of brainstem dysfunction that produces this response in humans may be similar, as in most cases decerebrate posturing is associated with disturbances of ocular motility. However, electrophysiologic, radiologic, or even postmortem examination sometimes reveals pathology that is largely confined to the forebrain and diencephalon. Thus, decerebrate rigidity is a clinical finding that probably represents dysfunction, although not necessarily destruction extending into the upper brainstem. Nevertheless, it represents a more severe finding than decorticate posturing; for example, in the Jennett and Teasdale series, only 10% of comatose patients with head injury who demonstrated decerebrate posturing recovered.
Thus erectile dysfunction drugs gnc purchase levitra oral jelly 20 mg with mastercard, this effect might be characteristic of inhalable particulate matter and might not depend solely on the manganese content of the particle impotence 21 year old buy levitra oral jelly 20 mg amex. A number of reports indicate that oral exposure to manganese erectile dysfunction medicine with no side effects order 20mg levitra oral jelly free shipping, especially from contaminated water sources impotence caused by medications purchase 20 mg levitra oral jelly free shipping, can produce significant health effects. These effects have been most prominently observed in children and are similar to those observed from inhalation exposure. An actual threshold level at which manganese exposure produces neurological effects in humans has not been established. However, children consuming the same concentration of manganese in water as adults are ultimately exposed to a higher mg/kg-body weight ratio of manganese than adults (as a consequence of the lower body weight of children as well as their higher daily consumption volume and greater retention of manganese). While many of the studies reporting oral effects of excess manganese have limitations that preclude firm conclusions about the potential for adverse effects, these studies collectively suggest that ingestion of water and/or foodstuffs containing increased concentrations of manganese may result in adverse neurological effects. The available studies on the effect that manganese has on fertility (as measured by birthrate) is inconclusive. Two studies in men occupationally exposed to manganese show adverse effects on reproductive parameters: one found increased sexual dysfunction and the other found reduced sperm quality, but neither measured birthrate in wives of affected workers. Impaired sexual function in men may be one of the earliest clinical manifestations of manganese toxicity, but no dose-response information is currently available, so it is not possible to define a threshold for this effect. There is a lack of information regarding effects in women since most data are derived from studies of male workers. Developmental data in humans exposed to manganese by inhalation are limited and consist mostly of reports of adverse pulmonary effects from inhaling airborne manganese dust and adverse neurological effects in offspring following ingestion exposure. Animal studies indicate that manganese is a developmental toxin when administered orally and intravenously, but inhalation data concerning these effects are scarce and not definitive. Some studies in children suggest that routine exposures to high levels of manganese from contaminated drinking water may ultimately impair intellectual performance and behavior. The few available inhalation and oral studies in humans and animals indicate that inorganic manganese exposure does not cause significant injury to the heart, stomach, blood, muscle, bone, liver, kidney, skin, or eyes. Studies in pigs have revealed a potential for adverse coronary effects from excess manganese exposure. Although no firm conclusions can be drawn from the mixed results in animal studies, there are little data to suggest that inorganic manganese is carcinogenic. It should be noted that individuals with cirrhosis of the liver, as well as children with a congenital venous anomaly known as a portosystemic shunt, may be at heightened risk of health deficits from exposure to dietary and environmental sources of manganese. Manganese is ordinarily eliminated from the body through bile, but cirrhosis and portosystemic shunts impair the normal functioning of the liver and thus limit the ability of the body to excrete manganese, which then can accumulate in the blood and, eventually, the brain. There is clear evidence from studies of humans exposed to manganese dusts in mines and factories that inhalation of high levels of manganese can lead to a series of serious and ultimately disabling neurological effects in humans. This disease, termed manganism, typically begins with feelings of weakness and lethargy. As the disease progresses, a number of other neurological signs may become manifest. Although not all individuals develop identical signs, the most common are a slow and clumsy gait, speech disturbances, a masklike face, and tremors. The neurological symptoms may improve when exposure ceases; however, in most cases, the symptoms are found to persist for many years post-exposure. In addition, a syndrome of psychological disturbances (hallucination, psychosis) frequently emerges, although such symptoms are sometimes absent. As the disease progresses, patients develop severe muscle tension and rigidity and may be completely and permanently disabled. Workplace inhalation exposure levels producing overt symptoms of manganism have been on the order of 222 mg manganese/m3. In addition, manganism patients sometimes have psychiatric disturbances early in the disease, a propensity to fall backward when pushed, less frequent resting tremor, more frequent dystonia, a "cock-walk", and a failure to respond to dopaminomimetics. Subclinical neurological effects have been observed in numerous studies of workers exposed to manganese dusts at lower exposure levels than those associated with symptoms of overt manganism. These effects include decreased performance on neurobehavioral tests; significantly poorer eye-hand coordination, hand steadiness, and reaction time; poorer postural stability; and lower levels of cognitive flexibility.
Generic 20mg levitra oral jelly. MENS ED ERECTILE DYSFUNCTION: ACOUSTIC WAVE CARE.